What is the anomaly scan?
The 20-week ultrasound is also known as the anomaly scan. The main objective of the scan is to determine whether the development of the child’s structures and organs are taking place normally. This is a detailed scan typically done between 18weeks and 20 weeks of gestation during which each part of the fetal anatomy is examined to see if the baby is developing normally. Special attention is paid to the brain, face, spine, heart, stomach, bowel, kidneys and limbs. Another observation that would be made is whether there is sufficient amniotic fluid.
Examples of physical defects that can be revealed by a 20-week ultrasound include: spinal cord defects, improper formation of the skull, accumulation of fluid in the brain, heart defects, a hole or rift in the diaphragm, a hole or rift in the abdominal wall, missing or malformed kidneys, missing or malformed bones, malformed arms and legs.
When will the anomaly scan be done?
The anomaly scan is done between 18 and 20 weeks (second trimester). In addition to this scan, the obstetrician may ask more scans if:
- The patient is carrying twins or more.
- The anomaly scan showed a low lying placenta.
- The patient had spotting or bleeding from the vagina.
- The anomaly scan revealed problems that need to be monitored.
- The patient has a medical condition such as diabetes or hypertension.
- The patient has a history of premature labour or late miscarriage.
Will the scan provide 100% confirmation of the structural development?
While a majority of babies are born healthy, a small percentage stands the risk of developing complications. Even a normal anomaly ultrasound scan is no guarantee of a healthy child as some defects will not show up on the ultrasound. The procedure by itself does not pose any risk to the mother or child.
What will the fetal medicine specialist examine?
The specialist will examine all the baby's organs and take measurements. These include:
- The shape and structure of the baby's head. At this stage any impairment in the brain development is visible.
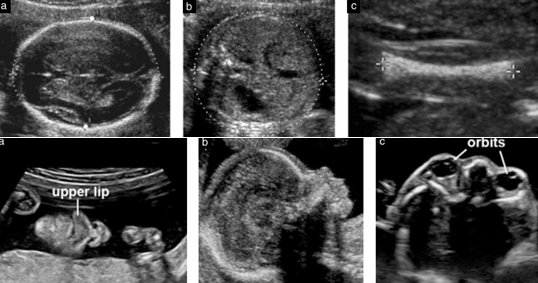
- The baby's face to check for a cleft lip. But cleft palates inside a baby's mouth are hard to see and are not often picked up.
- Rarely, amniocentesis may cause amniotic fluid to leak.
- The baby's spine, both along its length, and in cross section, to make sure that all the bones align, and that the skin covers the spine at the back.
- The baby's abdominal wall, to make sure it covers all the internal organs at the front, as well as check the placenta, umbilical cord and the amniotic fluid
- The baby's heart. The top two chambers (atria) and the bottom two chambers (ventricles) should be equal in size. The valves should open and close with each heartbeat. The specialist will also examine the major veins and arteries which carry blood to and from the baby’s heart.
- The baby's stomach. Amniotic fluid swallowed by the baby is visible in the ultrasound as being present in the stomach
- The baby's kidneys. The specialist will check if both kidneys are present and if urine flows freely into the bladder. If the baby's bladder is empty, it should fill up during the period of the scan itself.
- The baby's arms, legs, hands and feet. The specialist will look at the baby's fingers and toes, but not count them
The placenta will be described as low if it reaches down to or covers the mouth of the uterus (the cervix). If the placenta is lying low in the uterus, the patient will have another scan in the third trimester to check its position. By then, it's likely the placenta will have moved away from the cervix.
It is possible to count the three blood vessels (two arteries and a single vein) in the umbilical cord, but it is not routine procedure.
The level of amniotic fluid for the baby to move freely will be checked.
Also parts of the baby's body will be measured, to gauge the growth. The measurements include:
- Head circumference (HC)
- Abdominal circumference (AC)
- Thigh bone (femur) (FL)
The measurements should match up to what's expected for the baby, depending on when the due date is.
Fetal medicine specialists have a list of conditions to look out for. In ‘mid trimester anomaly scan’ (18 to 22 weeks as per ISUOG guidelines), only the fetal parts mentioned in the scan report have been evaluated. Parts of fetus not mentioned in the report are not evaluated in a routine scan. For eg. counting of fingers/toes, assessment of external ears, palate etc.
Abnormal conditions are either very serious, which may mean that a baby can't survive, or they may be treatable conditions, once the baby is born.
If the condition is treatable, the fetal medicine specialist will collaborate with the obstetrician to enable adequate care once the child is born.
Can Down syndrome or chromosomal abnormalities be seen on the scan?
This scan can also identify 50% to 60% of cases of Down syndrome, but the First Trimester Screening (FTS) test is definitely better for this.
Because a portion of cases of Down syndrome appear normal on ultrasound, only an amniocentesis (testing the fluid surrounding the baby for its chromosomes) can give this information for certain.
Sometimes babies with chromosomal abnormalities have signs called ultrasound markers. These include in order of importance thick skin behind the neck (nuchal fold), absent nasal bone, mild fluid within the ventricles of the brain, aberrant subclavian artery in the neck, occasionally short arms or legs. While some babies with chromosomal abnormalities have these markers, it is important to remember that many normal babies also have these signs. The only way to diagnose or exclude a chromosomal problem for certain is to have an amniocentesis.
Limitations of the scan
- Though the 18-20 week scan can detect when certain parts of the baby's body have grown abnormally, it may not be possible for clinicians to identify why it has happened or make a firm diagnosis based on the scan alone. Sometimes doctors will wait to give the baby more time to develop and carry out repeat scans. It is important to remember that a normal ultrasound does not always mean the baby will be born without any abnormalities.
- Generally the earliest time to look for birth defects is between 18 and 20 weeks of pregnancy however, some will not become evident until late in the pregnancy. Anatomic areas such as the heart, the face and the hands are difficult to assess and not all defects are detectable.
- Other factors such as the patient’s build, scars from a previous operation and the way the baby is positioned may limit the diagnostic ability of this test.
- Some conditions, including heart defects and bowel obstructions, may not be seen until later in the pregnancy. Having an anomaly scan will most likely rule out all these conditions.
- Certain anomalies like delayed sulcation of the brain can be diagnosed only after 24 to 25 weeks of gestation, and hence in certain cases a repeat anomaly scan may be advised.
- Some anomalies like soft tissue fusion of fingers/toes, absence of anal opening or absence of auditory opening may not be recognizable by ultrasonography.
- Late onset/evolving anomalies like congenital diaphragmatic hernia/ hydrocephalus/ microcephaly/ club foot/ certain heart abnormalities/kidney& intestinal obstructive anomalies etc may not be picked up in mid trimester scan.
- Study of the genital organs is prohibited under the PC & PNDT Act. Hence detection of abnormalities of the genital organs is not feasible.
- Despite a protocol driven, detailed study, some anomalies can be missed in prenatal Ultrasound scan, Under some circumstances a normal ultrasound finding may be misinterpreted as an anomaly. These are due to limitations of ultrasound/fetal position.
- Some findings may not be anomalies but may necessitate serial scan follow up, biochemical testing or invasive testing. Some findings may be transient and may change with time.
- Specialized Fetal Echo (heart study) or extended neuro sonography (brain study) will be done if the referred doctor requests for the same. Even if the brain may look normal on ultrasound examination, its function cannot be evaluated.
- Even in a specialized fetal echocardiography (heart study), certain cardiac anomalies such as secundum ASD, small VSD, PDA and other subtle anomalies cannot be picked up.
- Several factors like gestational age at which scan is done. Fetal position at the time of scan, maternal body habitus, liquor volume and shadows from fetal parts may restrict/limit visibility. The study may then necessitate repeat scans
- Obesity is a special challenge for ultrasonography. The fat in the mother’s abdominal wall absorbs the ultrasound energy, thus degrading the images and making the diagnosis very difficult.
- Chromosomal anomalies cannot be diagnosed on ultrasound scans alone. Ultrasound markers, if noted will only increase the risk of the fetus having chromosomal abnormalities and will warrant further evaluation. Karyotyping (chromosomal study of fetus by invasive testing with needle) is the confirmatory test. Such a needle/invasive test will carry a risk of procedure related pregnancy loss which will be discussed when necessary by the doctor.
- 3D/4D ultrasound is used only to assess certain abnormalities and not as a routine.
- Multiple gestations (twin/triplet pregnancies etc.) may cause difficulties in ultrasound examination due to fetal position and overlap.
What if there are signs of a problem on my scan?
If the 20-week ultrasound reveals any abnormalities, the consequences to the child may not yet be clear. The patient will be offered the option of follow-up testing. Any defect(s) revealed during the original test will then be examined in further depth. The patient may also be offered the option of undergoing an amniocentesis procedure.
